
MRCO BLOG
Medical Musings, Health Hypotheses & Therapeutic Thoughts
|
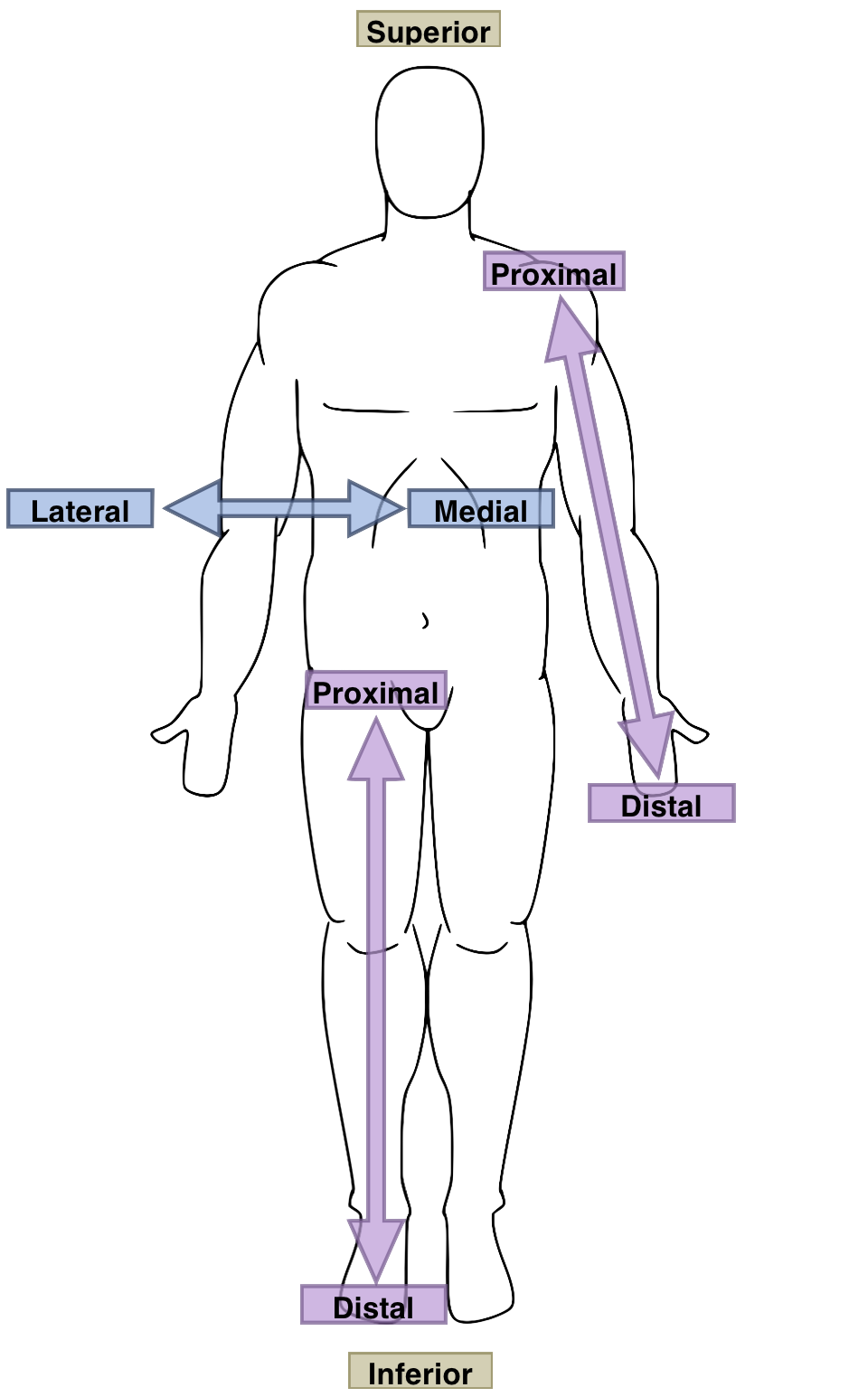
Finally, we will consider some of the common causes of lateral knee pain. You may remember from the last blog that lateral means 'away from the mid-line of the body', so this is pain on the outside of the knee. Many of the structures on the outside of the knee are similar to those on the inside, so they do not need much further consideration here (if you haven't yet, I strongly recommend that you read the first few posts about the knee, as they provide some much-needed background and context) These include: Lateral meniscal injuries e.g. tears
17/12/2018 Common Causes of Knee Pain, Pt IIIn the last blog, we considered some common causes of pain in the front (anterior) and back (posterior) knee.
3/12/2018 Common Causes Of Knee Pain Pt ISo, we have discussed how the poor 'design' of the knee joint means it is prone to various injuries and dysfunctions, but what does that mean in your everyday life? Here we will consider the anatomy of the knee a bit further, and discuss some of the ways our knees can give us grief. It is important to remember that, like most of the other joints in the body, the knee requires its neighbours to be doing a relatively good job in order to perform its own.
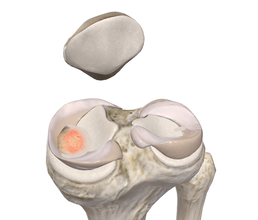
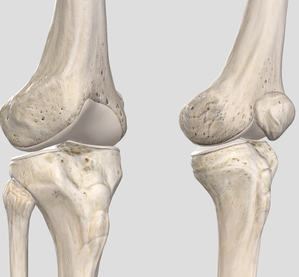
Dr. Edmund Bruce-Gardner The knee is a pretty badly-designed joint. Evolution doesn't move towards perfection, but function. As bipedal (two-legged) creatures who evolved from quadrupedal (four-legged) ones, quite a few compromises and fudges have been made. [The shoulder is another good example. it is a heavily-modified hip (i.e. ball-and-socket joint), but one where the bony shape and supporting ligaments have to allow for such a large range of motion that it relies on the surrounding muscles for nearly all of its support and integrity, as well as on the function of all the other joints surrounding it. You can read more about the weird and wonderful world of the shoulder complex here.] But anyway, the knee... It is a hinge joint, the largest joint in the body, sandwiched in between the two longest bones in the human body, the femur (thigh bone) and tibia (shin bone). This is a fairly bad idea to start with, because long levers generate a lot of force. Worse, it's not a very simple hinge joint. If it were, and could only bend forwards and backwards, and we wouldn't be able to walk on broken or uneven ground. So we have the longest bones (/levers), generating a huge amount of force, going into the largest joint, which is also extremely complex.  Doesn't look massively stable, does it? Doesn't look massively stable, does it? Back when we put all of our weight through four ‘knees’ instead of two, this was less of an issue. We also tend to weight-bear with our knees more or less unbent. This provides a lot more opportunity for trauma. Contrast this with other mammals such cats, dogs, horses, chipmunks, etc. etc. The bottom of the thigh bone is a bit like the cartoon version of a bone, with two knobbly bits (called condyles) at the bottom. These then (theoretically) meet, or articulate, with the relatively flat top of the shin bone. This works about as well as you would imagine. 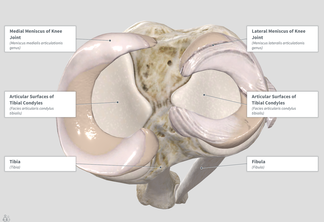 Evolution’s workaround here was to put these two sort of cups, called menisci, on the top of the flat bit of the shin bone (rather poetically called the tibial plateau). These allow the knobbly condyles to sit a bit more firmly on the top of the tibia. Now, of course, we have another structure that takes a lot of force, and can get injured. Most sports fans (not to mention players) will have heard of a torn meniscus. I tore mine when I was about fourteen, and still remember it as one of the most exquisitely painful experiences of my life. As you can see in the diagram above, when the menisci (the 'C-shaped' things around the outside) are in place they cover most of the top of the tibial plateau. 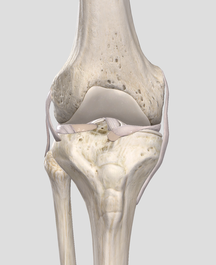 Here you can see the collateral ligaments (on the sides) and sneak a peek of the cruciate ligaments and menisci (between the femur and tibia) Here you can see the collateral ligaments (on the sides) and sneak a peek of the cruciate ligaments and menisci (between the femur and tibia) But wait! There's more! It's not all about the menisci. In a flash of evolutionary genius, the other main way that the knee is stabilised is by four... ...elastic bands, Well, not literally, but they might as well be. The rubber bands (known as ligaments by the medical types) are actually just thickenings of the capsule that surrounds the joint. Again, sports buffs will probably recognise the terms medial and lateral collateral ligaments. These refer to the ligaments on the inside, and outside, of the knee, respectively. The anterior and posterior cruciate (or 'cross-like') ligaments go between the femur and tibia, and can be seen (along with the menisci) sandwiched in there on the left. So we have this large, unstable joint subject to huge forces, that we hold in biomechanically-compromised positions. Hmmmm, what could go wrong?
All joking aside, we will go into some of the ways the knee (and associated structures) can start breaking bad. Stay tuned for my series on the knee, which will hopefully be completed at a slightly less glacial pace than the shoulder! |
AuthorsDrs. Edmund Bruce-Gardner and Soraya Burrows are osteopaths Categories
All
|

Osteopathy at Moreland Road Clinic
High quality & personalised service from experienced professionals. A safe, effective & collaborative approach to patient care. All osteopaths undertake a 4-5 year university degree and are licensed and registered healthcare pracitioners. |
Find Us
Moreland Road Clinic 85 Moreland Road Coburg VIC 3058 P (03) 9384 0812 F (03) 9086 4194 osteopathy@morelandroadclinic.com.au |
Popular Blog Posts
|
|
|
Osteopathy at Moreland Road Clinic is on Moreland Road, near the corner of Nicholson Street/Holmes Street, on the border of Coburg, Brunswick & Thornbury.
This makes Osteopathy at Moreland Road Clinic the ideal location for people in the inner north and outer northern suburbs of Melbourne, including: Coburg, Coburg North, Coburg East, Brunswick, Brunswick East, Brunswick West, Fawkner, Oak Park, Glenroy, Preston, Pascoe Vale, Pascoe Vale South, Gowanbrae, Hadfield, Essendon, Moonee Ponds, Thornbury and Reservoir. |
 RSS Feed
RSS Feed
11/2/2019
1 Comment