
MRCO BLOG
Medical Musings, Health Hypotheses & Therapeutic Thoughts
The question then becomes “OK, I understand that pain is an output, and is influenced by all these different factors separate to the signals coming form the body. But what can I do about my chronic pain??”
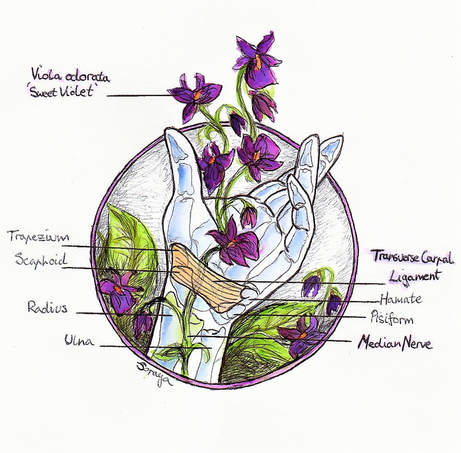
The human hand is such a sensitive and specialised structure; anatomically complex and strategically engineered by time and nature, having the ability to create such varied and precise movements. Our hands contain so many weird and wonderfully specialised sensory cells that function to collect information via touch, position, pressure or temperature in relation to our current surroundings. The information is continuously relayed to our brain where the appropriate networks of neurons pass precise instructions via the spinal cord, neural networks and down the nerves in our arms to the muscles responsible for generating the gestures we require. This intricate sensory/motor control system is continuously checking itself and making small adjustments. We could be typing away in an attempt to conquer the monstrous, multi-headed hydra-like inexhaustible queue of office emails, operating an electric sander to remove tired paint in an effort to restore an antique to its former glory or just the general lifting and carrying as we go about our everyday activities. With all these moving parts and capabilities made possible with our hands, we can create works of art and express ourselves. .
When we’re limber and feeling good, we barely notice how much we rely on and require that normal baseline level of ease. However, when things don’t go as planned and if an injury occurs, whether caused by simple tasks or other health conditions, the loss of our normal function is very apparent. One possible common condition responsible for hand pain is Carpal Tunnel Syndrome (CTS). It affects 4-5% of the population (1) and can be quite disruptive, affecting a variety of people, from pregnant women, office workers and the elderly, to tradesman and others who work directly with their hands. It seems to be caused by multiple factors, which could include (2);
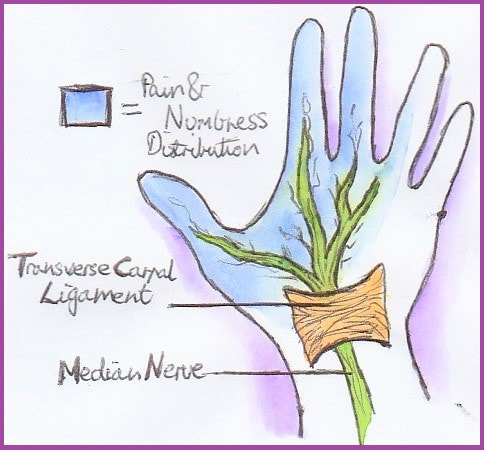
Many of the structures that operate the hand are sandwiched together and must pass through a channel at the wrist (the carpal tunnel) bordered by sturdy carpal (or wrist) bones and ligaments, particularly the transverse carpal ligament as the ‘unyielding ceiling’. Most of the space in this channel is occupied by rigid tendons that control finger movements, leaving only a small potential space for the squishy median nerve, which can be easily compressed here (1, 2). Being the main sensory and motor supply for the palm of the hand, a squished median nerve can result in the frustrating and restrictive experience that Carpal Tunnel Syndrome is known for. 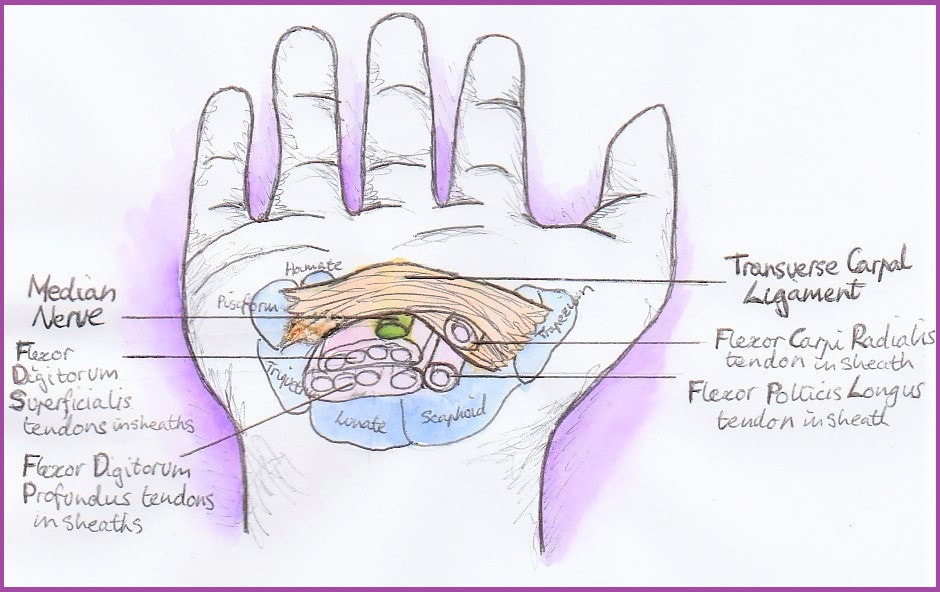 If you are experiencing signs and symptoms such as those described, the best course of action is to consult your GP or manual therapist as early as possible. This could limit the impact on your everyday life activities and the need for any interventions in future. If CTS is left to progress, a cortisone injection may be beneficial. It was reported that approximately 75% of patients experience improvement following this procedure (4, 5). Failing that, a small surgical procedure can be recommended. It involves releasing the transverse carpal ligament (the mentioned ‘ceiling’ of the carpal tunnel), creating more space for the muscle tendons to glide together at the wrist, alleviating the direct pressure placed on the median nerve. Luckily surgical intervention for CTS has a very high success rate, with over 90% of patients reporting alleviation of symptoms (6, 7, 8), However, it is important to remember that as far as your body is concerned, there is no such thing as 'minor' surgery! Even in the best case scenario, the carpal tunnel now has (even more rigid and unyielding) scar tissue around it, which can cause other issues. So the best thing to do is avoid any intrusive interventions. And it’s entirely possible!
Along with osteopathic techniques for treatment, there are some simple and inexpensive things to try, some examples include (2, 3);
 Developing an understanding of how and why this is happening; knowledge alone can alter the experience and help settle the worry. Being informed is a powerful position to be in as you can select the best course of action and knowing what the possible benefits or disadvantages of the available options are. CTS can be debilitating and impact negatively on your health and wellbeing and day-to-day activities. That’s why getting treated as soon as possible is so important. By finding the right combination of strategies that are best for you, your osteopath can get you moving and back into your daily routines, whether it be gardening, writing, creating a masterpiece, or tackling a home renovation. Not to mention going back into battle with inexhaustible email queues – the multi-headed hydras! References:
9/10/2018 What is Chronic Pain?NOTE: This blog post is essentially a copypasta of the page on the same topic; but it is so important a subject I wanted to make the information was available to all of our blog subscribers as well... Chronic PainWhen we talk about 'chronic pain', we're not just talking about pain that has been going on for a long time; although that it is part of the definition. Chronic pain, in this sense, involves changes to the way that information is carried and processed in our bodies. To understand this a little better, we will have to consider (briefly!) the nature of pain and what it means. Pain is an output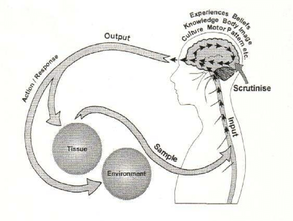 From Gifford (1998) From Gifford (1998) What this means is that all pain is produced by your central nervous system; that is, pain is the label your brain applies to information it really wants you to pay attention to. When you injure yourself, like burning your hand on a hotplate, your nerves send signals up to your spinal cord and brain. We call this nociception, or something like 'detection of something harmful or noxious'. Your brain then decides whether or not to call those signals 'pain'. From this point of view, the pain itself is just as real in something like phantom limb pain (when you (e.g.) have an arm amputated but can still feel pain in the hand) as when you accidentally stab yourself in the thigh while cutting a recipe out of a magazine (just a random example that sprang to mind). So pain is not something you feel in your body, it is something that is created and projected out by your brain. Put simply, it is an output, not an input. Pain is an evolutionary strategy In the case of touching your hand to a hot stove, you have already started moving your hand away by the time you feel the pain. What the pain is intended to do is to point out to you that your unprotected hand is not the best way to turn that pancake, and that maybe next time you should use a spatula! So the memory of pain makes us less likely to try and use our digits as kitchen utensils in the future as well as making us stop the behaviour causing the pain in the first place. It also makes you take care of an area while it is healing, so serves a protective function. So pain is just a warning signal, and in normal circumstances, it is a good thing. Another way of saying this is that it is a adaptive strategy, or one that makes you more likely to stay alive. People who can't feel pain for one reason or another run a very real risk of ignoring a seemingly small injury that then becomes infected, and possibly life-threatening. Pain is normal! Image by Studio224 Image by Studio224 Leading on from the above two points, it should be clear that pain is a normal function of our bodies when everything is working as it should, albeit one most of us don't really want! It is meant to be unpleasant, otherwise it wouldn't work the way it does. Pain is what we experience when our brains have decided we are threatened or in danger, and wants us to do something about it. In the case of chronic pain, where the pain has persisted long past the point where we might have expected any injury to heal, the key is to identify why the brain feels threatened. 'Pain' is, tellingly, also used with respect to grief or loss, or loneliness. This emotionally-laden 'pain' is crucial in understanding chronic pain - indeed, all pain! - as it reinforces the idea that these sensations are the result of many different inputs, and our emotions, thoughts, beliefs and behaviours are all important contributors to how we experience pain. Pain and damage are not necessarily related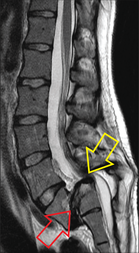 This image is from an asymptomatic 32 year old female. The red arrow shows where the spine has slipped forwards, the yellow points to the spinal cord doing a slalom around the step like an Olympic skiier! From Eliott et al (2010) This image is from an asymptomatic 32 year old female. The red arrow shows where the spine has slipped forwards, the yellow points to the spinal cord doing a slalom around the step like an Olympic skiier! From Eliott et al (2010) This starts to explain the idea that pain is an output, where trauma or tissue damage is not the only factor (as mentioned over on the page on age-related conditions like arthritis.) We know from decades of medical imaging that people can have the most spectacular structural failures, like compression of the spinal cord or broken bones, and experience little to no pain or dysfunction. Sheehan (2010) for example, found that among asymptomatic (i.e. not having any symptoms) 60 year-olds, over 90% had degenerative or bulging discs. 21% had spinal stenosis, narrowing of the hollow middle bit of the spinal column, where your spinal cord sits. One might imagine that squishing your spinal cord would result in some sort of symptoms, but not necessarily! See the image on the left for a truly mindboggling scan of a compressed spinal cord that did not result in any pain at all (they had the scan done for other reasons). Anecdotal reports from wounded in wartime often describe bullet wounds and even severe trauma as an impact, like being bumped or knocked in a crowd. At the other end of the spectrum, consider a paper cut. If pain is just an evolutionary mechanism to warn you about damage, why does the bloody thing hurt so much! It is not deep, or (under normal circumstances) anything close to a serious danger to the body, but we react as if it was the next thing to losing a limb. Chronic Pain
 So how can osteopathy help? An analogy I often use with my patients is to think about your central nervous system (or CNS, consisting of your brain and spinal cord) as a genius four year-old. It is incredibly discriminating and intelligent in some ways, and unsophisticated and stupid in others. Like a four year-old, it also has a tendency to throw tantrums (overreact with pain, for example). And also like a four year-old, the best way of getting through to it is repetition. By repeatedly moving and stretching areas where the body perceives pain, we can increase the 'positive feedback' coming from that area. "Look, we are moving this painful shoulder in all these different ways, and the arm has not fallen off! Maybe it's OK to decrease the number of pain labels we are attaching to this area. Maybe it's OK to relax a little!" This makes the CNS feel a little safer. We can also help you with some of the other facets of your pain. The folks over at NOI (the neuro-orthopaedic institute) have come up with this wonderful concept of DIMs ("Dangers In Me") and SIMs (Safeties in me) that can help identify unhelpful and helpful factors in your life that influence whether or not you feel pain. The more factors we can identify, the more chance we have of helping you get your CNS to a place where it feels safe, and where you do not feel pain. References Eliott, JM, Fleming, H & K Tucker (2010) "Asymptomatic spondylolisthesis and pregnancy" J Ortho Sports Phys Ther 40:324 Gifford, LS (1998) "Pain, the tissues, and the nervous system: a conceptual model" Physiotherapy 84(1):27-36 Sheehan, NJ (2010) "Magnetic resonance imaging for low back pain: indications and limitations" Ann Rheum Dis 2010; 69:7-11 Special mentions to The Sensitive Nervous System (Butler et al, 2000) and Explain Pain Supercharged (Butler et al, 2017), which are great resources around explaining both central and peripheral nueropathic pain and have informed my whole approach to chronic pain management.  .Headaches can be tricky. There are a lot of reasons to get headaches, these are divided into categories. Primary Headaches These are headaches that are not caused by some underlying medical condition, so they are benign (non-life threatening), although migraine sufferers may disagree! More than 90% of headaches fall into this classification. These include: Tension-type headaches (TTH) - the most common cause of headaches. It has been estimated that up to 90% of headaches are TTH. Migraines - the second most common primary headache. We do not yet fully understand why migraines occur, but current thinking is that they are caused by an interaction between nerve/brain and blood vessel abnormalities. Cluster headaches - extremely severe, sufferers who are mothers have often described the pain as worse than childbirth. Again, we are not sure what causes them, but it seems it may be something to do with a region of the brain called the hypothalamus. Cervicogenic (meaning coming from the neck) headaches. Secondary Headaches Result from trauma or some other underlying medical condition, such as infection, tumours, or bleeding in the brain. These account for less than 10% of headaches, but some causes may be life-threatening. Early diagnosis of these causes is important to avoid life-threatening complications. Your osteopath is trained in recognising the different types of headaches, and will refer you on to the appropriate specialist if there is any concern that you may be suffering from a secondary headache. However, let us assume that you have had your headache assessed by an appropriate healthcare professional. When that headache strikes, what can you do? Read on for our self-help tips and tricks...  1. Rest in a quiet, preferably dark, room This can be effective for migraines, as well as TTH/cervicogenic headaches. As stress is one of the biggest factors in many headaches, having a rest can help both with the stress, and help tense, tired muscles to relax. TTH and migraine sufferers are also often overly sensitive to sound or light (or both). Sit or lie down in a quiet, darkened or dimly-lit room. Try to relax the muscles of the neck, shoulders and back.  2. Have a glass of water Dehydration can cause headaches, or make them worse. Keep yourself well hydrated to avoid these (and for a host of other reasons as well!). Remember, by the time you feel thirsty, you are already dehydrated. As little as 2% loss of body water content can cause loss of mental alertness and bodily fatigue, and it has been estimated that many of us do not even notice our thirst until we are moderately dehydrated (6-10% of body water). (For reference, above 15% is considered severe dehydration, and may even result in death)  3. Breathing/Relaxation exercises These work on the same principle as resting in a darkened room, by helping to reduce stress and muscle tension. Take several deep, long breaths. As you breathe out, feel tense and sore areas relax and get heavy. Bonus points for imaging a peaceful scene (go to your happy place!).  4. Simple stretches and movements. Phew. This is a big category, so we are only going to give a few examples. If you want more exercises that are tailored to you and your issue, ask your osteopath at Moreland Road Clinic about a personalised exercise program! (a) Drop your chin down towards your chest, then slowly rotate your head in a half circle, first one way, then the other. Do not put your head backwards, as this compresses the joints in the neck, and tenses the very muscles we are trying to relax. (b) Bend your head gently to the side. You want to feel a gentle pull in the muscles on the side of the neck. You can use your hand to help guide the head, but do not pull on it strongly or sharply. (c) You can also intentionally (gently) contract muscles to help them relax. Think of it as bringing them a bit more back under conscious control. This is very effective in exercise (b), above. When you (e.g.) take the head off to the side, gently push back against the controlling hand. Do not use more than 5-10% of your strength - the point is to engage the muscles, not make them work hard. You can do the same thing, gently pressing your forehead into the palm of your hand (This will help relax the muscles in the front of the neck), or the base of the skull backwards into your hand (for the muscles at the back). (d) Lie on your back, with a rolled up towel where your skull meets the top of your neck. Tuck your chin in, and gently press your head down onto the towel. Your should feel stretching and gentle pressure in the head/neck junction. (e) Roll your shoulders in nice wide, slow circles. This helps to stimulate blood flow to the tight, sore muscles around the shoulders, upper back and neck, and will help them relax. 5. Self-massage Another big topic! We will only give a few examples here. For more techniques, ask your osteopath for advice... Self-massage is often difficult as it is hard to reach the areas you need to. However, headaches are probably one of the best issues to self-massage, as you should be able to reach most parts of your head and neck (if you can't, maybe you should book an appointment with your friendly neighbourhood osteopath to look at your shoulder problem!). Use the finger pads (flats), not the tips - you want a nice, comfortable sensation, nothing too 'poke-y'. (a) Describe gentle circles on your temples, the muscles above the ears (Yes! You have muscles there! You may have noticed them if you have ever smiled too hard for too long), and the side of the jaw. Target any particular painful spots, you will probably find they are tender to the touch as well. Keep it gentle! (b) Place your thumbs near the base of your skull. Find the thick columns of muscle that run just on either side of the spine, and slide off them to the outside. You should feel these little depressions (hollows) where the neck meets the base of the skull. Press inwards and upwards until you feel a bit of discomfort. Using the pads of your thumbs, massage gently in small circles (keeping the inwards and upwards pressure). (c) You can also try lifting your scalp up away from the head - if you have long hair, this is easy. Take a broad clump in each hand and gently lift upwards. You should feel almost instant relief. Combine with some gentle circular movements (again, with the finger pads) over the scalp, paying special attention to the sore bits. NOTE: If you have a willing accomplice, get them to do these exercises for you. That way, you are not using the muscles in your shoulders and arms, which will make the techniques more effective. 6. Try heat and/or cold A hot shower, or moist heat to the back of the neck may help to relieve the symptoms of tension headaches. Alternatively, try a cold pack (Always wrap cold packs in a towel or similar, so there is nothing too cold making direct contact with the skin) placed on the sore spots (e.g. temples, forehead, base of skull). If either of these are uncomfortable/hurt, stop! The aim here is to reduce pain!  7. Over-the-counter (OTC) medication A quick note: osteopaths are not qualified to give advice on drugs in general, so always consult your doctor or pharmacist about any medications you want to take. Over-the-counter (OTC) drugs such as ibuprofen (e.g. Nurofen), paracetemol (e.g. Panadol), sodium diclofenac (e.g. Voltaren), naproxen sodium (e.g. Naprogesic) and aspirin may all help with headache pain. Interestingly, caffeine seems to make the effects of some of these more effective and rapid, which is why many OTC medications include it. However, please note that caffeine may be a trigger for migraines in sufferers. Also note that using any headache medication for more than three days in a week may cause medication-overuse headaches (these would be secondary headaches). Please consult your GP if you find you are needing medication this often.  8. Acupuncture Without going into too much detail, there are broadly speaking two main methods of acupuncture for headaches. Traditional Chinese acupuncuncture involves placing fine needles in specific points around the body. These points may be anywhere (i.e. not necessarily close to your head, in the case of headaches), and are chosen based on the idea that pain, dysfunction and disease are due to energy imbalances in the body. Trigger point dry needling (the technique used at Moreland Road Clinic) uses the same needles (and often techniques), but the points chosen are in tight and sore muscles that your therapist has identified as contributing to your headache pattern (so will normally be around the head, neck, shoulders and upper back). Research indicates that these needles stimulate blood flow to the area, helping tense muscles relax, and may also help to release endorphins, the body's natural painkillers; both of which can help with headaches, particularly TTHs.  9. Exercise
Anyone who knows me and my treatment approach has probably been wondering when this one would sneak in! Research indicates that moderate exercise can help reduce the number and intensity of headaches (and by the same token, lack of exercise can predispose towards chronic headaches). This is probably because exercise is another way of releasing those endorphins (those wonderful pain-killing chemicals!), as well as promoting good overall health. Stronger muscles don't have to work as hard to do their normal job (this includes the heart as well!), and a more efficient cardiovascular system (heart, lungs, blood vessels etc) reduces the stress and strain on your body in general. Aim for 150 minutes (two and half hours, or half an hour five days a week) of moderate intensity exercise, something that (a) gets your heart rate up a bit and (b) you enjoy! (b) is really important - if you do not enjoy it, you are less likely to maintain a long-term regime. Finally, I would like to talk about when to see your doctor about your headaches. Please contact your healthcare professional if: -your headaches are extremely frequent, or start increasing in frequency, or last more than a few days. - Please seek advice if your headaches are accompanied by change in co-ordination or balance, fits, faints, blackouts, seizures, confusion, blurred/double vision, numbness, severe nausea or vomiting, dizziness or vertigo, fever, stiff neck, or shortness of breath. - If your headache is sudden, severe, occurs immediately after an accident (especially head trauma), or is "the worst you've ever had", seek immediate medical attention. Dr. Edmund Bruce-Gardner, Osteopath Please note, you should not rely solely on books/the internet/my mate Jim at the pub for your health information. Please do not use this information to diagnose or treat yourself, and seek medical advice for any symptoms that concern you. The aim of these blogs is to increase peoples' self-reliance and ability to self-manage, but always assumes you are doing so in collaboration with your healthcare team. Like our blog? Click these links to like us on faceook, review us on google, or sign up to our mailing list 6/8/2016 Chronic pain, ain't no gain!Chronic pain, ain't no gain! But it doesn't need to always be this way. While pain clinics are fantastic, they often have long wait lists 😕 Luckily the osteopathy & psychology team at Moreland Road Clinic can help get back into life again!💃🏼💃🏼💃🏼  |
AuthorsDrs. Edmund Bruce-Gardner and Soraya Burrows are osteopaths Categories
All
|

Osteopathy at Moreland Road Clinic
High quality & personalised service from experienced professionals. A safe, effective & collaborative approach to patient care. All osteopaths undertake a 4-5 year university degree and are licensed and registered healthcare pracitioners. |
Find Us
Moreland Road Clinic 85 Moreland Road Coburg VIC 3058 P (03) 9384 0812 F (03) 9086 4194 osteopathy@morelandroadclinic.com.au |
Popular Blog Posts
|
|
|
Osteopathy at Moreland Road Clinic is on Moreland Road, near the corner of Nicholson Street/Holmes Street, on the border of Coburg, Brunswick & Thornbury.
This makes Osteopathy at Moreland Road Clinic the ideal location for people in the inner north and outer northern suburbs of Melbourne, including: Coburg, Coburg North, Coburg East, Brunswick, Brunswick East, Brunswick West, Fawkner, Oak Park, Glenroy, Preston, Pascoe Vale, Pascoe Vale South, Gowanbrae, Hadfield, Essendon, Moonee Ponds, Thornbury and Reservoir. |




 RSS Feed
RSS Feed
18/11/2019
0 Comments