
MRCO BLOG
Medical Musings, Health Hypotheses & Therapeutic Thoughts
The question then becomes “OK, I understand that pain is an output, and is influenced by all these different factors separate to the signals coming form the body. But what can I do about my chronic pain??” The first answer seems maddeningly unhelpful. Just because you intellectually “understand” something, does not mean that you understand it, in the sense of knowing it and believing it ‘in your bones’. So the first thing you have to do, is go back and re-read all the stuff you just finished about pain being an output, multi-factorial, and not related to damage. Think about it: if someone describes to you how you play a tennis shot, for example, you might well understand what they are describing, but I very much doubt you will be on Centre Court at Wimbledon next year! Sometimes a different way of explaining things can click where previous elucidations were, well, as clear as mud! So try to read as many different accounts of pain and how it works as you can.
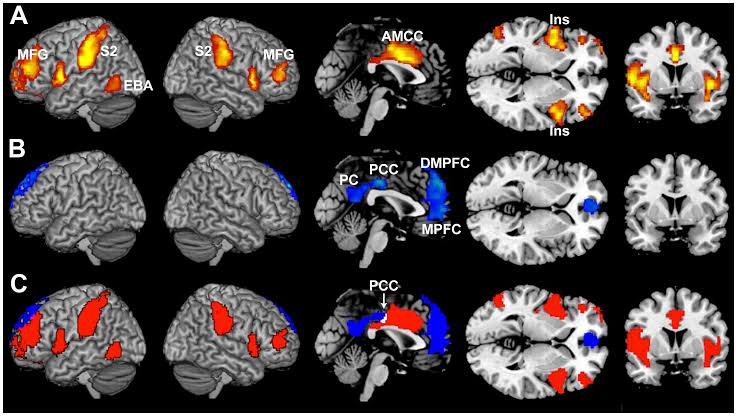
Others are interactions between various parts of the brain with very long, complicated names like rostroventromedial medulla or anterior cingulate cortex, leading to a complex relationship between areas involved with emotion, cognition, motivation and sensation. It’s all very complicated, and the thing to remember is that these other influences can both facilitate (increase) or inhibit (decrease) the strength of the signal that we identify as pain. The second really important point is that these factors are much, much stronger than the original signal itself, like a couple of hundred times stronger!
Note: these ideas of ‘petrol’ and ‘water’ are functionally identical to the notions of DIMS and SIMS used the NOI group, as described in the previous chronic pain blogs. So whatever the signals are coming up from the body, whether or not we see them as pain depends on a whole host of other factors. Remember our axiom from the previous blogs: Pain is the label your body attaches to something when it feels it has more [credible] evidence of threat, than of safety. The more we learn about how pain works, the smaller part those original signals seem to play when it comes to the brain ‘deciding’ what is credible evidence. If you have more buckets of water than petrol, no pain; and vice versa. So, whatever else, you don’t need to worry that the pain is just in your head. Well, except that your brain is inside your head (it would be worrying were it not). Dammit, you know what I mean. So there are physical things going on, but these are influenced and modulated by well, pretty much everything else. Many of the brain sites identified as being involved with the processing of noxious stimuli are generally involved with emotional systems. It’s been said before, but it bears repeating: How you think and feel about your pain changes the way you feel your pain. It stands to reason, then, that if we change the ways we think and feel about our pain, the way we feel the pain will also change! So it might seem frustrating, because you already feel you’ve done all of this to death, what with the specialist, your osteo, the occupational therapist, and pain management clinic (if you’ve gotten that far) all banging on about the need for education and understanding. On a side note, if all of these disparate professionals all agree on something, that’s worth sitting up and taking note in and of itself! Consensus in science is a good thing, it doesn’t indicate conspiracy But speaking purely personally, as my understanding of pain, and my issues, has developed and deepened over the years, there is less and less… …emotional content, I suppose, attached to it. I tend to perceive it much more as my body trying to tell me something (whether or not its concern is justified is a different story!), rather than that gut-wrenching sensation of wrongness. So again, as redundant as it seems, step one really is going back and reading, and re-reading, everything you can find (and understand! The research itself can be pretty heavy going!) on pain and the brain. Ask your osteopath for some resources if you feel like you need a some inspiration and a fresh approach! The next blog will deal with Step Two, where we start putting some of this theory into practice. References
[1] The biochemical and neuroendocrine bases of the hyperalgesic nocebo effect. Benedetti F, Amanzio M, Vighetti S, Asteggiano G J Neurosci. 2006 Nov 15; 26(46):12014-22. [2] Nocebo hyperalgesia: how anxiety is turned into pain. Colloca L, Benedetti F Curr Opin Anaesthesiol. 2007 Oct; 20(5):435-9. [3] Isolating the modulatory effect of expectation on pain transmission: a functional magnetic resonance imaging study. Keltner JR, Furst A, Fan C, Redfern R, Inglis B, Fields HL J Neurosci. 2006 Apr 19; 26(16):4437-43. [4] Wood P, Schweinhardt P, Jaeger E, et al. Fibromyalgia patients show an abnormal dopamine response to pain. Eur J Neurosci. 2007;25:3576–3582 [5] Baliki MN, Geha PY, Fields HL, Apkarian AV. Predicting value of pain and analgesia: nucleus accumbens response to noxious stimuli changes in the presence of chronic pain. Neuron. 2010;66:149–160. [6] Baliki M, Petre B, Torbey S, et al. Corticostriatal functional connectivity predicts transition to chronic back pain. Nat Neurosci. 2012;15:1117–1119. Leave a Reply. |
AuthorsDrs. Edmund Bruce-Gardner and Soraya Burrows are osteopaths Categories
All
|

Osteopathy at Moreland Road Clinic
High quality & personalised service from experienced professionals. A safe, effective & collaborative approach to patient care. All osteopaths undertake a 4-5 year university degree and are licensed and registered healthcare pracitioners. |
Find Us
Moreland Road Clinic 85 Moreland Road Coburg VIC 3058 P (03) 9384 0812 F (03) 9086 4194 osteopathy@morelandroadclinic.com.au |
Popular Blog Posts
|
|
|
Osteopathy at Moreland Road Clinic is on Moreland Road, near the corner of Nicholson Street/Holmes Street, on the border of Coburg, Brunswick & Thornbury.
This makes Osteopathy at Moreland Road Clinic the ideal location for people in the inner north and outer northern suburbs of Melbourne, including: Coburg, Coburg North, Coburg East, Brunswick, Brunswick East, Brunswick West, Fawkner, Oak Park, Glenroy, Preston, Pascoe Vale, Pascoe Vale South, Gowanbrae, Hadfield, Essendon, Moonee Ponds, Thornbury and Reservoir. |



 RSS Feed
RSS Feed
18/11/2019
0 Comments