
MRCO BLOG
Medical Musings, Health Hypotheses & Therapeutic Thoughts
 Picking up where we left off last time..... We were discussing the intricacies of the shoulder complex, and its relationship with surround body structures and areas. We noted that the shoulder is extremely mobile, with very little in the way of bony congruency (stability from the shape of the joint(s), and hence relying on the supporting musculature. 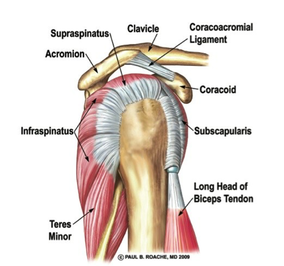 A particularly important group of these is known as the rotator cuff, so called because they form a cuff around the top of the arm bone and are (surprise surprise!) responsible for arm rotation. 54% of asymptomatic (i.e. not having pain or problems) patients aged 60 years or over were found to have partial or complete tears of the rotator cuff on MRI (a type of imaging), which should give you some idea of how hard those poor little fellows work over the course of our lives. So why does the rotator cuff have to work so hard? As previously mentioned, the shoulder is an incredibly mobile [series of] joint[s], and allows incredible mobility, but at the expense of stability. 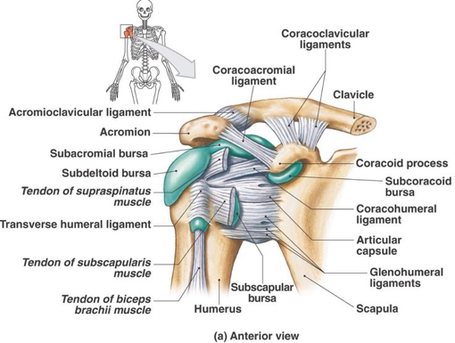 There is a fibrous capsule surrounding the shoulder joint proper (the glenohumeral joint), as there is around many/most of the joints in the body. In the shoulder, this fibrous layer is both thin and loose, allowing a wide range of movement. The tendons of the rotator cuff blend with and reinforce this fibrous layer of the joint capsule, helping to protect and stabilize the joint. Although they all have separate functions (some turn the arm out and the shoulder, others inwards etc.), the rotator cuff muscles work as a group to hold the head of the humerus (top of the arm bone) in the glenoid fossa (remember I described the shoulder as not so much of a ball-and-socket, but as a ball-and-tiny-saucer?). The glenoid fossa is the technical term for that little saucer-shaped depression) during arm movements. They also passively support the dependent (hanging) humerus while sitting or standing, especially supraspinatus. The arm would dislocate downwards out of this socket were it not for the rotator cuff (and the angle of the fossa). They also work with the bigger deltoid muscle to lift the arms out to the side. In short, the rotator cuff helps us to support the shoulder and control fine movements that then enable us to use the wonder of evolution, the hand, and lets your move your arms around over your head without everything smashing together. 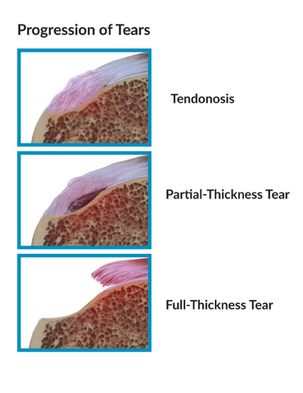 Common injuries of the rotator cuff Rotator cuff overuse issues start early in life, with oedema (swelling) and haemorrhage (bleeding) of the tendon and bursa. This can start before the age of twenty five. Stage II involves fibrosis and tendinitis, that is, the thickening and scarring of connective tissue (a general term that includes tendons, ligaments, cartilage, bone, and even fatty tissue and blood, but for these purposes refers to the tendons of the muscles) and inflammation/irritation and degeneration of the tendons. This broadly speaking takes place from the ages of around 25-40 years of age. Stage III involves tearing of the rotator cuff, which can be either partial or full-thickness tears, and typically takes place over the age of 40. Additionally, rotator cuff pathology is often bilateral (both sides), even when one side only is symptomatic (painful), and those with one painful side have been shown to be at risk of developing pain and tear progression on the other side (see refs at bottom of page). This is possibly related to compensatory overuse of the non-painful side. It is also possible to have an acute or sudden-onset tear, often caused by a fall onto an outstretched arm, or trying to lift/catch something unexpectedly heavy. These may occur with or without the above-mentioned changes over time. 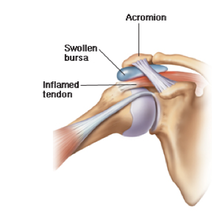 Bursitis is when a small fluid-filled sac that is designed to cushion from shock/friction itself gets irritated or infected. The most common bursitis in the shoulder of the subacromial bursa. Impingement syndrome happens when outer end of the shoulderblade, called the acromion, contacts or impinges on the tendon, bursa, or both. Primary impingement is due to structural issues (i.e. how we are built). Some of us have smaller sub-acromial spaces than others. Osteoarthritis (wear and tear) can make this worse due to little bony spurs called osteophytes that further reduce this space. Secondary impingement is normally a result of dynamic instability (i.e. how we use our shoulders). If the rotator cuff muscles are weak, they do not do their job well; so are unable to prevent the head of the humerus from riding up into the sub-acromial space as we lift our arm. This also leads to pinching of the tendon and/or bursa. Of course, inflamed/swollen tendons and bursae also take up more room, further decreasing the potential sub-acromial space, so these problems can co-exist and reinforce each other. 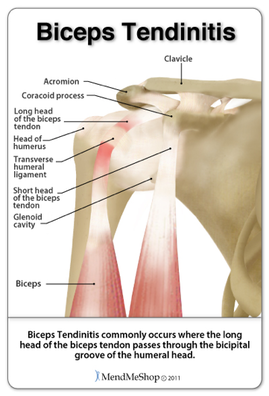 An Honourable Mention… goes to bicipital tendinopathy, which is inflammation/irritation of the long head of biceps tendon or its sheath. It is rarely seen in isolation, and normally co-exists with rotator cuff pathology/impingment or other shoulder issues. Like the above, it is normally caused by overuse/degenration, shoulder instability, tendon impingment or trauma. Stay tuned to our next blog installment on the shoulder, treatment.. References
[i] Mall NA, Kim HM, Keener JD, et al. Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables. The Journal of bone and joint surgery American volume. 2010;92(16):2623–33 [ii] Moosmayer S, Tariq R, Stiris M, Smith HJ. The natural history of asymptomatic rotator cuff tears: a three-year follow-up of fifty cases. The Journal of bone and joint surgery American volume. 2013;95(14):1249–55 |
AuthorsDrs. Edmund Bruce-Gardner and Soraya Burrows are osteopaths Categories
All
|

Osteopathy at Moreland Road Clinic
High quality & personalised service from experienced professionals. A safe, effective & collaborative approach to patient care. All osteopaths undertake a 4-5 year university degree and are licensed and registered healthcare pracitioners. |
Find Us
Moreland Road Clinic 85 Moreland Road Coburg VIC 3058 P (03) 9384 0812 F (03) 9086 4194 osteopathy@morelandroadclinic.com.au |
Popular Blog Posts
|
|
|
Osteopathy at Moreland Road Clinic is on Moreland Road, near the corner of Nicholson Street/Holmes Street, on the border of Coburg, Brunswick & Thornbury.
This makes Osteopathy at Moreland Road Clinic the ideal location for people in the inner north and outer northern suburbs of Melbourne, including: Coburg, Coburg North, Coburg East, Brunswick, Brunswick East, Brunswick West, Fawkner, Oak Park, Glenroy, Preston, Pascoe Vale, Pascoe Vale South, Gowanbrae, Hadfield, Essendon, Moonee Ponds, Thornbury and Reservoir. |
 RSS Feed
RSS Feed
18/8/2017
1 Comment