
MRCO BLOG
Medical Musings, Health Hypotheses & Therapeutic Thoughts
|
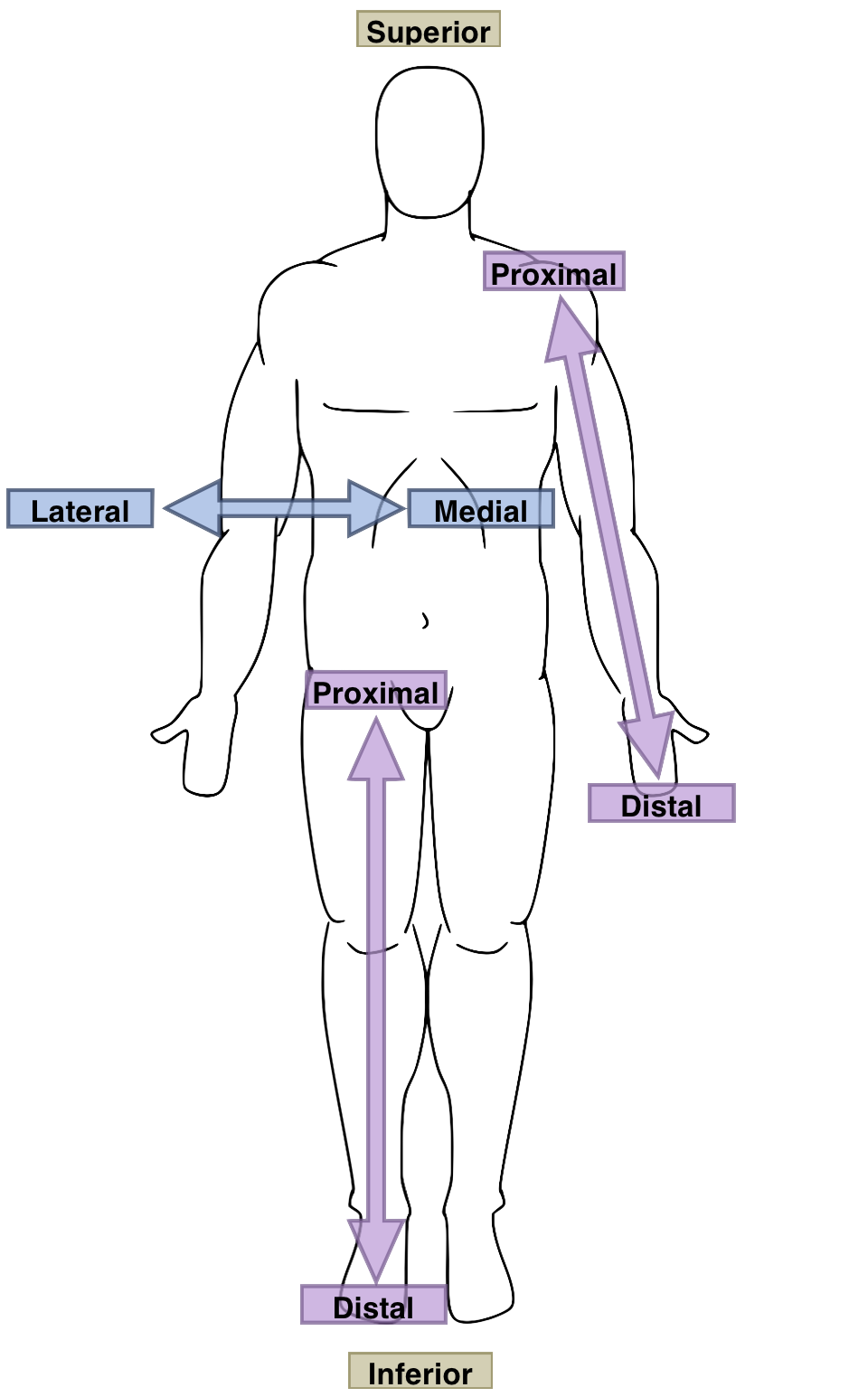
In the last blog, we considered some common causes of pain in the front (anterior) and back (posterior) knee.
Pain in the knee may, as you have already guessed if you have been following our blogs, be referred from distant areas, most notably the low back; or (rarely) be related to another underlying disease process. For brevity's sake, we will be focusing on local structural issues, but for a full understanding of your issue, an analysis of your foot, ankle, hip and low back structure and function will likely be required. Medial Knee Pain Pain on the inside of the knee may be related to a number of issues, some more common in one stage of life (e.g. childhood/adolescence), and some in others. Medial meniscal issues
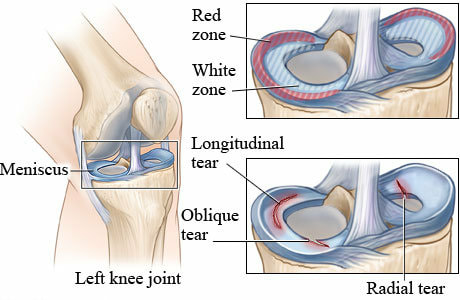
In younger patients, this is more likely to be a traumatic onset, normally involving a twisting motion on a bent, weight-bearing knee (very common in football - sorry! 'Soccer', as you tend to say here!). Incidence of these injuries tend to peak at around 20-29 years of age. In older patients, it is more likely to be due to age-related degeneration. We see the difference between these in the type of injury: the traumatic injuries often involve vertical or oblique tears from the shearing force involved; while degenerative tears are often horizontal, the result of layers of connective tissue separating, or delaminating (Lamina means 'sheet' or 'plate' in Latin). In either case there may be clicking and/or locking, as swelling, pain or a torn meniscal fragment prevent the knee from fully straightening (or bending too far). Depending on where the tear is, it may heal on its own (the 'red zone' in the image above, which receives a blood supply. so is much more likely to be able to heal) or require surgery (the 'white zone'). It is worth noting that meniscus injury hugely predisposes you towards osteoarthritis of the knee. This also applies to inappropriate surgical treatment (they actually use meniscal surgery to give lab animals knee arthritis quickly so they can study it). Luckily, our knowledge of and attitude towards meniscal injury and surgery has improved massively over the last thirty years or so. Guess when I had my torn menisci and operations - the early nineties :-( Osteoarthritis (OA) of the medial compartment of the knee
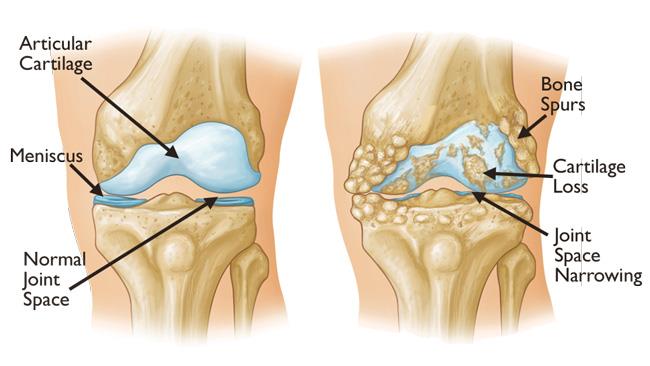
Note: Changes in the way that the joint moves means that force is shifted from areas of cartilage that are adapted for loading to those that are less well-suited to it, changing the way we walk. This accelerates the process of degeneration. This means that gait modification, that is, learning how to walk differently (and more efficiently), has the potential to reduce pain and slow the progress of OA (Vincent et al, 2012). If osteoarthritis is the most common form of arthritis (it is - it is most common cause of disability in the United States, for example), then you can imagine how common the most frequently-affected area must be. That's right! It's the medial compartment of the knee! Also note that there is (unfortunately) nothing stopping you from having both medial and lateral compartment OA of the knee, but medial is much more common. And as always, things are necessarily that simple. As anyone familiar with these blogs is likely to have picked up, damage and pain are not necessarily directly related. Just because you have a knee xray that shows some loss of cartilage - or even apparent bone-on-bone - is not necessarily cause for alarm. Like our knowledge of and approach to meniscal issues, our methods of dealing with knee arthritis have become much more nuanced. While surgery may eventually be necessary, it is by no means a certainty. Ask your osteopath what you can do to help manage your knee arthritis. Medial Collateral Ligament (MCL) injury
Pes Anserine Burisitis
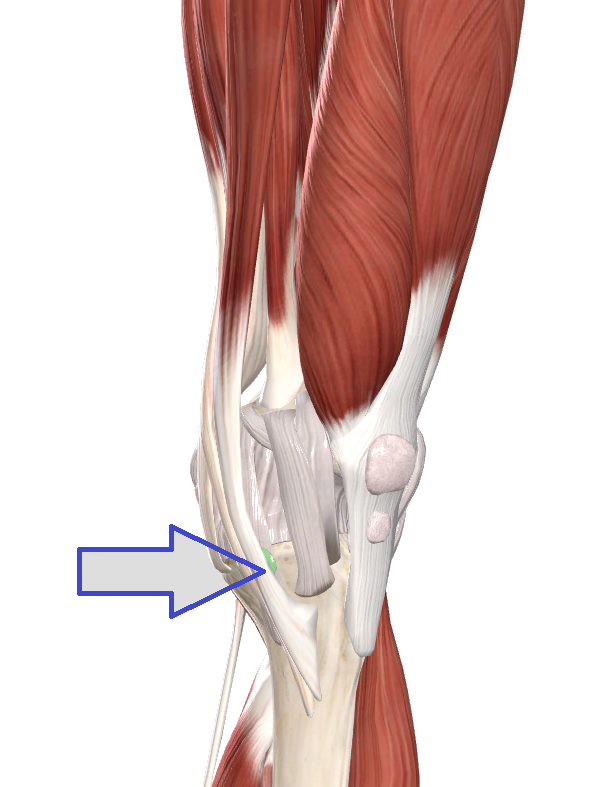
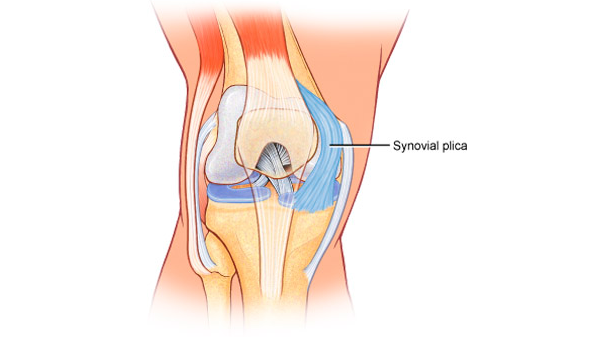
Pain from pes anserine bursitis can typically be felt a few centimetres below and back from the knee-cap, on the inside (the medical lingo would be inferomedial to the patella). There may be local swelling (oedema) and redness, and it will be tender to the touch. Medial (or Tibial) Collateral Ligament Bursitis This is irritation of a bursa that lies deep to the MCL, between the ligament and the meniscus, and between ligament and tibia. (Medial) Plica Sydrome
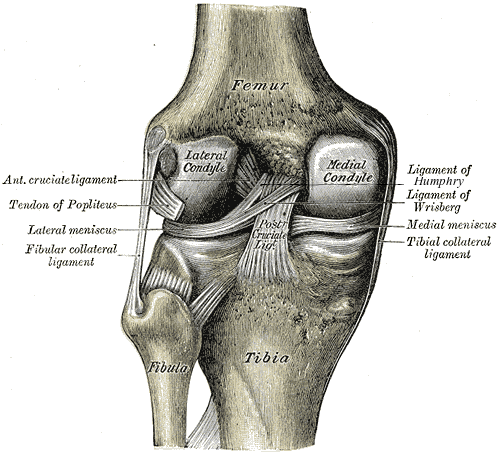
You may be able to see, in the image above, how the plica might rub or 'snap' over the bony medial condyle of the femur with repeated flexion (bending). Other factors that may lead to Plica Syndrome include other altered knee motion (such as consequent to ankle or hip problems); blunt trauma, such as an impact to the inside of the knee; or irritation of the fat pad to which the plica attaches. Often, plica syndrome occurs alongside other knee issues, such as meniscal tears, patellar tendonitis or Osgood-Schlatter's disease. So those are the most common causes of medial knee pain. Phew! That ended up being a little longer than anticipated. Rather than overloading you with too many diagrams and anatomical minutiae, we will save the causes of lateral knee pain for next time. See you then! Leave a Reply. |
AuthorsDrs. Edmund Bruce-Gardner and Soraya Burrows are osteopaths Categories
All
|

Osteopathy at Moreland Road Clinic
High quality & personalised service from experienced professionals. A safe, effective & collaborative approach to patient care. All osteopaths undertake a 4-5 year university degree and are licensed and registered healthcare pracitioners. |
Find Us
Moreland Road Clinic 85 Moreland Road Coburg VIC 3058 P (03) 9384 0812 F (03) 9086 4194 osteopathy@morelandroadclinic.com.au |
Popular Blog Posts
|
|
|
Osteopathy at Moreland Road Clinic is on Moreland Road, near the corner of Nicholson Street/Holmes Street, on the border of Coburg, Brunswick & Thornbury.
This makes Osteopathy at Moreland Road Clinic the ideal location for people in the inner north and outer northern suburbs of Melbourne, including: Coburg, Coburg North, Coburg East, Brunswick, Brunswick East, Brunswick West, Fawkner, Oak Park, Glenroy, Preston, Pascoe Vale, Pascoe Vale South, Gowanbrae, Hadfield, Essendon, Moonee Ponds, Thornbury and Reservoir. |
 RSS Feed
RSS Feed
17/12/2018
0 Comments